
Chapter 1 - Anatomy of the GU Tract and Histology of GU Tumours
WHO Blue Book Tumors of the Urinary System, 2004. Eble J, Epstein J, Sesterhenn I, Sauter G (Eds). Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs (IARC WHO Classification of Tumours). The International Agency for Research on Cancer. Lyon: IARC Press, 2004
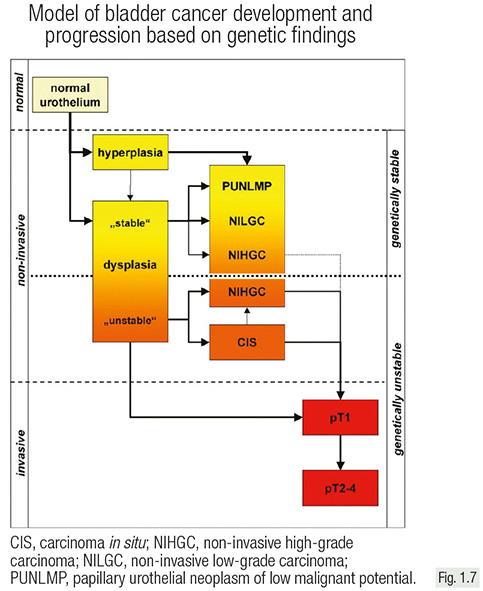
Development and progression of urothelial neoplasia occurs through two quite different genetic pathways.
Non-invasive papillary cancers of low/intermediate grade (pTa, G1/2) develop from dysplasia/hyperplasia and almost never progress to invasive cancer.
Invasive carcinomas are mostly of high grade and are mainly derived from carcinoma in situ or high-grade non-invasive papillary carcinomas (pTa, G3).

The classification of non-invasive papillary carcinomas is confusing because two “non-congruent” systems are typically used, either alone or in parallel.
Most clinicians are familiar with the WHO 1973 grading system that classifies non-invasive cancers as pTaG1, pTaG2, or pTaG3.
The WHO 2004 version (also adopted in the WHO 2016 version) also includes: papilloma, papillary urothelial neoplasm of low malignant potential (PUNLMP), non-invasive papillary cancer, low grade, and high grade non-invasive bladder cancer.
The clinical term ‘non-muscle invasive bladder cancer’ is used for pTa and pT1 tumours.

pTa and pT1 tumours not only represent two different entities at the genetic level, but also have a completely different clinical course.
While pTa tumours rarely progress, pT1 tumours are early stages of highly malignant neoplasms.
Revision Questions
- What are the two main groups of urothelial neoplasms?
- What is the difference between the WHO 1973 and WHO 2004/2016 classification?
- Why should the term “superficial bladder cancer” be avoided?
