
Chapter 1 - Anatomy of the GU Tract and Histology of GU Tumours
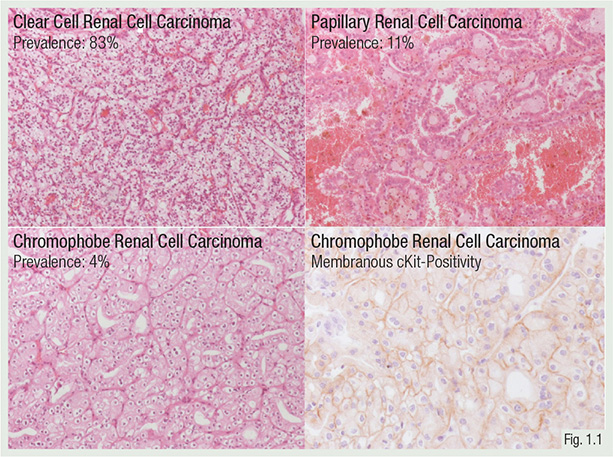
>95% of kidney cancers have a characteristic morphology that can be classified as: clear cell, papillary and chromophobe renal cell carcinoma (RCC), and collecting duct carcinoma.
A small proportion of rare kidney cancer entities are defined on a molecular basis, e.g. the microphthalmia transcription factor (MiT) family translocation RCC and succinate dehydrogenase-deficient RCC.
A 2018 study from Carlo et al showed a high prevalence of cancer-associated germline mutations in advanced kidney cancers (especially in non-clear cell RCC: 11.7% RCC-associated gene mutations).

Pathological tumour stage has a strong prognostic impact.
In the past, various grading systems (e.g. Thoenes or Fuhrmann) have been used for RCC staging. Today, the World Health Organization/International Society of Urological Pathology (WHO/ISUP) four-tiered system should be applied.
Tumour grade is defined mainly on the basis of nucleolar prominence.

Courtesy http://alf3.urz.unibas.ch/pathopic/intro.htm
5%-7% of kidney tumours are benign. Oncocytoma is the most frequent benign kidney tumour. The tumour is well circumscribed, mahogany brown with a central scar.
Angiomyolipomas represent 1% of kidney tumours. They consist of varying proportions of mature fat, thick-walled blood vessels, and smooth muscle.
Multilocular cystic renal neoplasm of low malignant potential is in principle a malignant tumour, but is entirely composed of cysts, with very few cancer cells. Metastases have not been reported.
Revision Questions
- What are the main subtypes of RCC?
- What is the best predictor of prognosis in RCC?
- Which carcinoma has the best prognosis?
