
Chapter 1 - Anatomy of the GU Tract and Histology of GU Tumours
More than 95% of all testicular neoplasias are germ cell tumours (GCTs). Germ cell tumours mostly occur at young age (peakfrequency at the age of 30 years).
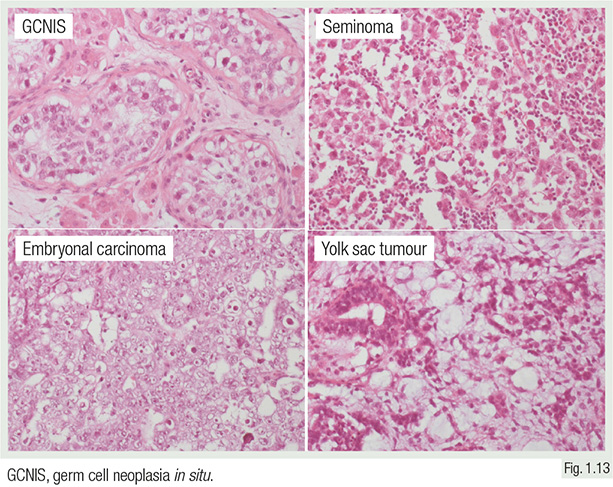
More than 90% of GCTs develop through germ cell neoplasia in situ (GCNIS), formerly called intratubular germ cell neoplasia, unclassified (IGCNU), which is commonly found in the vicinity of these cancers.
50% of GCNIS progress to invasive GCTs within 5 years, and at least 70% within 7 years.

Bostwick DG & Cheng L. Urologic Surgical Pathology, 3rd edition. New York: Elsevier, 2014
Seminoma is the earliest development stage of invasive GCT.
About 50% of all testicular GCT halt at that stage of development and are diagnosed as pure seminomas.
Teratoma in the adult is a “differentiated type” of germ cell tumour having evolved from GCNIS and seminoma. Teratoma in the adult is thus considered malignant.

Tumour stage (pT) is critical for subsequent therapy of testicular tumours.
Most pT2 stages are diagnosed because of vascular invasion.
Regional lymph nodes include the abdominal, para-aortic, preaortic, interaortocaval, precaval, paracaval, retrocaval, and retroaortic nodes.
Revision Questions
- What is the precursor lesion of most GCTs?
- What is the typical age of diagnosis for GCT?
- Why is a testicular teratoma in an adult considered malignant?
