
Chapter 1 - Anatomy of the GU Tract and Histology of GU Tumours
Prostate cancer is very common. A complete examination of the prostate will reveal cancer in 50% of men at the age of 50 and >75% at the age of 75 years.

Accordingly, precursor lesions are even more common in the prostate and many patients have more than one spatially separated PC.
Normal prostate epithelium is characterised by the presence of two cell layers: basal cells and acinar cells.
Prostate biopsy is the only tool for establishing a definitive diagnosis of PC.
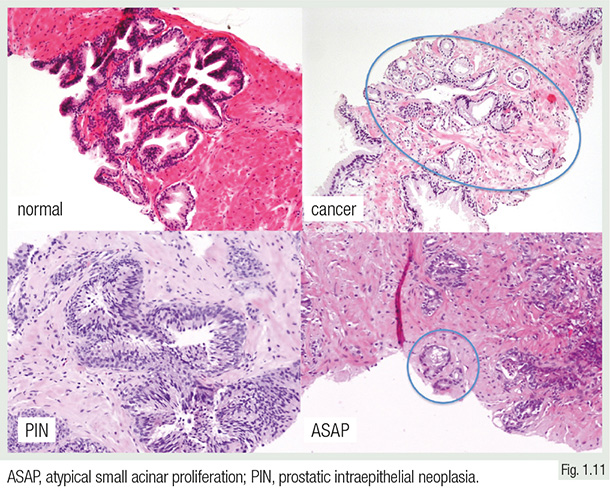
Findings in prostate biopsies include: normal, prostatic intraepithelial neoplasia (PIN), atypical small acinar proliferation (ASAP), and carcinoma.
PIN is the precursor lesion of prostate cancer. ASAP is a diagnostic category that includes all changes that are suspicious for cancer but not unequivocally diagnostic.

Srigley JR. Mod Pathol 2004;17:328-348
PC is entirely composed of atypical cells, while basal cells are completely lost. Gleason grade is the strongest predictor of tumour aggressiveness.
In contrast with all other grading systems, the Gleason grade is based solely on tumour architecture and does not consider any cytological changes.
The Gleason score is defined as the sum of the two most common grade patterns. The traditional Gleason grading system only distinguishes 5 groups: ≤6, 3+4, 4+3, 8, 9-10, also termed ISUP grade groups 1-5. The use of tertiary grades or the percentage of Gleason 4/5 offers a finer assessment of cancer aggressiveness.
Revision Questions
- What is the precursor lesion of PC?
- What is the meaning of “ASAP” and when is this term used?
- What is the characteristic of Gleason grading?
