
Screening and surveillance of malignant melanoma
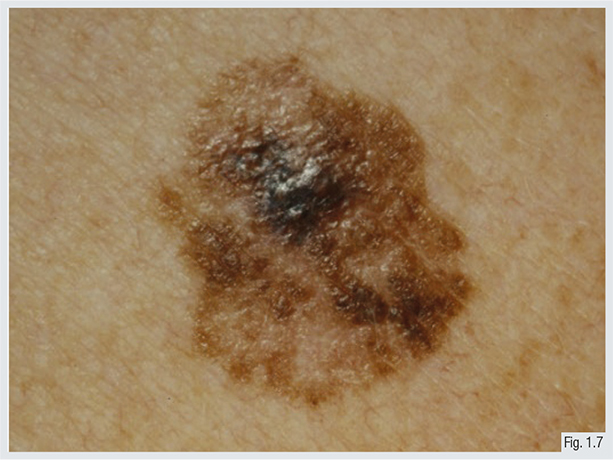
Awareness for self-examination of pigmented naevi using easily recognisable rules is underlined. One example is the ABCD rule for pigmented lesions: A-Asymmetry, B-Border, C-Colour, D-Diameter, helping to differentiate between benign and malignant lesions.
Patients at risk should be screened by total body skin examinations with a dermatoscope or comparable imaging technique (see Chapter 9).
Screenings should be performed by experienced physicians including mucous membranes and examination and palpation of lymph node stations.
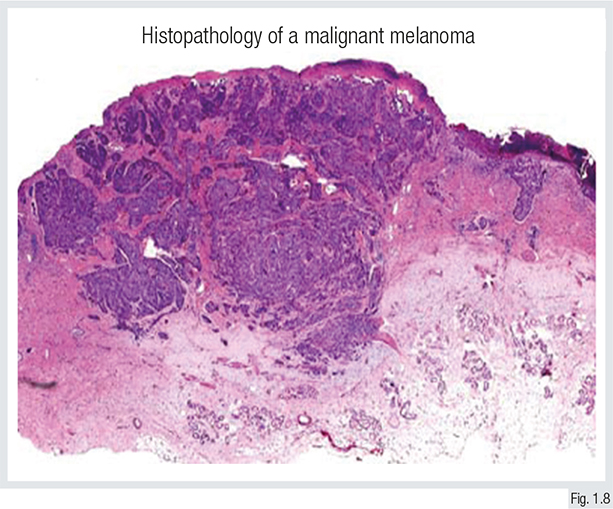
Suspicious lesions should be excised completely and examined histopathologically. If a melanoma is confirmed, further diagnostics and therapeutic options should be initiated.
Secondary prevention is established by a regular follow-up schedule including clinical examination and ultrasound.
For higher tumour stages, imaging techniques should be used to detect disease progression early and thus increase disease-specific survival.

Regular screening can lead to early detection of skin cancer with lower invasion and depth of the tumour, which is known to be a risk factor for worse prognosis.
Skin cancer screening programmes vary between countries, with regular investigations every 2 years from the age of 35 in Germany to no general regular screenings in the USA.
So far, a decrease in mortality attributed to skin cancer screening has not been detected. Still, potential benefitsmight be relative to quality of life or aggressiveness of treatment.
Revision Questions
- What does ‘C’ in the ABCD rule stand for?
- What does regular screening consist of?
- How is the diagnosis of melanoma confirmed and by whom?
