
Chapter 1 - Epidemiology, Risk factors and Pathogenesis of Squamous Cell Tumours

Transformation of normal mucosa into invasive HNSCC follows a molecular progression model of multistep carcinogenesis.
Loss of genetic material from chromosome region 9p21 and inactivation of p16 tumour suppression gene are the earliest alterations identified at transition to hyperplastic mucosa.
Subsequent transition to dysplasia is characterised by loss of 3p and 17p and by p53 inactivation. Loss of 11q, 13q and 14q precedes transition to carcinoma in situ.
Loss of 6p, 8p and 4q is identified during transformation to invasive HNSCC. Tobacco-related HNSCC is associated with mutation of p53 and downregulation of p16 protein.
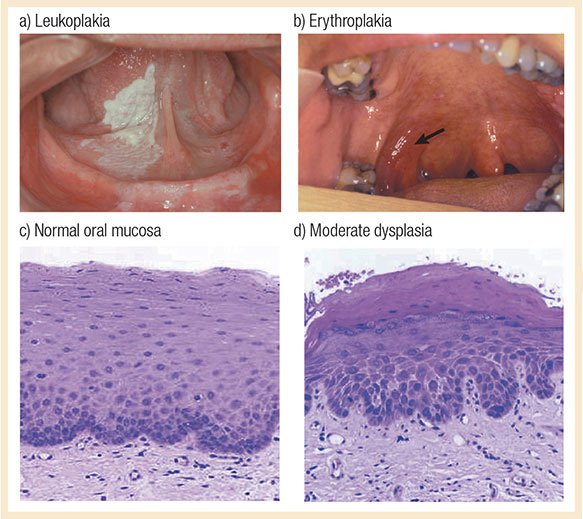
Leukoplakia and erythroplakia are the precursors of invasive HNSCC in the oral mucosa. Leukoplakia appears as white plaques and erythroplakia as a red zone of mucosa.
Field carcinogenesis refers to carcinogen distribution over large areas in upper aerodigestive tracts, due to continuous exposure, rendering mucosa a potential site for cancer.
HPV infection carcinogenesis: The integration of HPV DNA into the host genome disrupts the expression of factor E2, the transcriptional repressor of E6 and E7 viral proteins.

E6 and E7 encode oncoproteins that bind and degrade p53 and retinoblastoma (Rb) tumour suppressors, respectively. Degradation of Rb induces expression of p16INK4A.
Rb is a negative regulator of p16 protein; low Rb levels lead to p16 upregulation. HPV+ OPC is typically p53 and Rb1 wild-type and demonstrates high p16 protein levels.
Revision Questions
- Which molecular abnormalities are associated with tobacco-related HNSCC?
- What are the molecular features of HPV+ OPC?
- What are the premalignant lesions of invasive squamous cancer in the oral mucosa?
