
Chapter 1 - Histopathology of Gynaecological Cancers
Cervical cancer is the most serious complication of human papillomavirus (HPV) infection, particularly from some HPV types designated as “high-risk HPV” (mostly Types 16 and 18).
Two viral reading frames, E6/E7, deregulate reparative proteins, p53 and Rb, at cell cycle check points favouring genetic errors and malignant transformation.
The declining incidence of cervical cancer over the last decades is related to screening programmes that detect early cancers or precursor lesions. Vaccination is a new horizon for prevention.
FIGO staging: Stage I: limited to the cervix; Stage II: initial parametria/vagina; Stage III: deep infiltration parametria/vagina; Stage IV: bladder/rectum/distant metastasis.

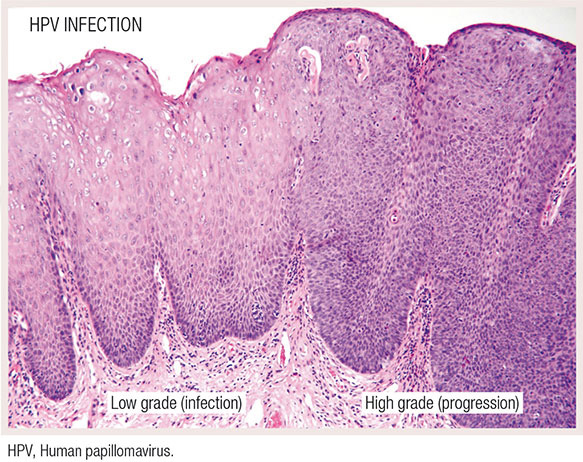
Squamous cell carcinoma accounts for 70% of cervical cancers. Pre-invasive lesion (cervical intraepithelial neoplasia, CIN) features include well-known condylomatous changes or low-grade CINs (multinucleation and perinuclear halos) and features suggestive of malignancy or high-grade CINs (marked cell atypia, and p16 positivity).
Invasive carcinoma is usually of the non-keratinising type.

Adenocarcinomas account for 20%–25% of cervical cancers and are difficult to detect by screening. Most are HPV cancers and HPV18 is frequent. Histological types include endocervical and mucinous; mixed adenosquamous carcinomas may occur.
Small cell undifferentiated carcinoma is the least frequent, but a highly aggressive, HPV cancer.
A few adenocarcinomas are not HPV related; they include gastric type mucinous and clear cell adenocarcinoma and adenocarcinoma arising from mesonephric remnants.
Revision Questions
- Why is the incidence of cervical cancer in developed countries decreasing? What is a promising discovery for reducing cervical cancer incidence even in developing countries?
- What are the most common, high-risk HPVs related to invasive cervical cancer? What is the molecular pathogenesis?
- What HPV-related features can be identified at cytology/histology?