
Organisational Infrastructures
Healthcare services are often organised in ‘silos’ – administratively, financially, professionally and culturally (Figure 1).
In integrated care, different specialists can provide their services regardless of these silos. Standardised care pathways are one methodology that may facilitate integrated care. In standardised care pathways, the patient course is planned individually based upon a common template. Interactions and critical events may be depicted. Standardised care pathways represent a means to overcome dependency on the individual physician’s practice for referral or intervention. However, standardised care pathways may also become a barrier to integration if they are perceived to limit the physician’s evaluations and adjustments.
Figure 1: Healthcare includes silos at different levels.
From: Kaasa S, Loge JH, Aapro M, et al. Integration of oncology and palliative care: a Lancet Oncology Commission. Lancet Oncol 2018; 19: e588-e653.
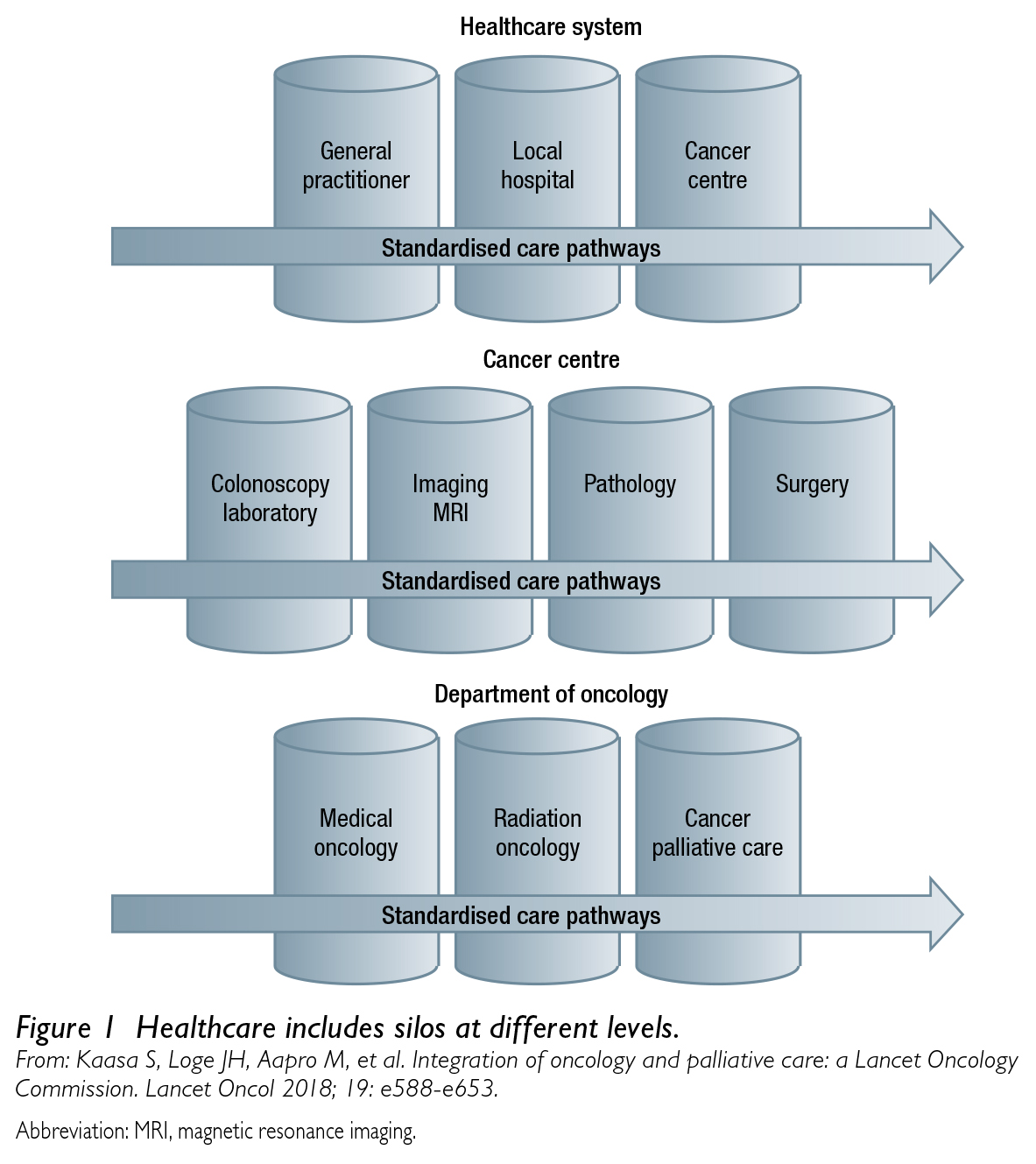
Abbreviation: MRI, magnetic resonance imaging.
Co-localisation of services facilitates contact and referral/communication between departments and individuals. Defining which services can be offered as out-patient and which must be in-patient can reduce hospitalisation, and technology for communication through electronic patient records, or other low-threshold mechanisms for contact between different levels of care (i.e. primary care, hospitals, nursing homes), should be established.
MDTs are organisational structures that coordinate healthcare by bringing together the many specialists involved, improving the quality of the provided care. The composition of MDTs in oncology often varies according to primary cancer type and the situation of the individual patient. Typically, oncology MDT representatives are surgeons, medical and radiation oncologists, radiologists and pathologists; it is uncommon to include palliative care specialists. For a patient-centred approach, palliative care specialists should be included in oncology MDTs. Also, palliative care MDTs should be implemented, further breaking down organisational silos by inviting relevant specialists from the oncology MDTs in addition to other pivotal professions in palliative care, such as physiotherapists, social workers, psychologists, occupational therapists, dieticians and chaplains. Potentially controversial, the patients and their caregivers could also be considered as members of the MDTs. Referral to palliative care MDTs should be based on predefined unacceptable symptom levels from systematic assessments, but appropriate time points for referral should also be defined in the standardised care pathways.
