

Definition
The advent of next-generation sequencing (NGS) allowed, for the first time, the read-out of large amounts of DNA in a faster and lower-cost way, compared to Sanger sequencing [1]. Thus, it became possible to detect multiple genetic alterations at the same time, using the same assay, leading to the concept of “multigene sequencing”. This can be applied in tumour tissue, but also in circulating tumour cells (CTCs), circulating tumour DNA (ctDNA) and in normal tissue (with constitutional DNA). Multigene sequencing is being increasingly performed in breast cancer patients, both in the early and in the metastatic settings.
Germline mutations
Multigene sequencing can identify many different genetic germline abnormalities (present in all the cells of the person), which can or cannot increase the risk of breast cancer. Nowadays, there are multiple commercial and academic breast cancer susceptibility multigene panels, which usually include high-penetrance genes, as well as moderate- and low-penetrance risk genes and genes of unknown significance. Yet, the number and type of genes included and the lab techniques employed change from panel to panel. Moreover, there is little consensus as to which genes should be included. There is a FDA-approved direct-to-consumer (DTC) BRCA1/2 test (the “23andMe” test [2]). Recently, the European Union has published a new general regulation on in vitro diagnostic medical devices, including predictive genetic tests, but it will come into force only by 2022 [3]. Yet, in Europe, there is no European Union or national legislation specifically regulating DTC genetic testing [4, 5]. Thus, medical guidelines recommend that patients should have comprehensive pre- and post-test counselling and provide consent for any type of cancer susceptibility multigene testing [1, 5, 6]. Furthermore, quality, data privacy and safety of these tests should be carefully monitored [5].
BRCA1 and BRCA2 were the first cancer susceptibility genes to be identified as increasing the risk for breast and ovarian cancers. If mutated, these high-penetrance genes confer a significantly higher risk of developing breast cancer, compared to the wild-type population: there is a lifetime cumulative breast cancer risk of 57-87% for BRCA1 mutation (5-8% in men) and of 41-84% for BRCA2 mutation [5, 7–11]. Later, other breast cancer high-penetrance genes have been identified, namely PALB2 (33-58% cumulative risk for breast cancer if mutated), PTEN (25%-85%), STK11 (45-50%), TP53 (54%) and CDH1 (39%-52% risk for lobular breast cancer).
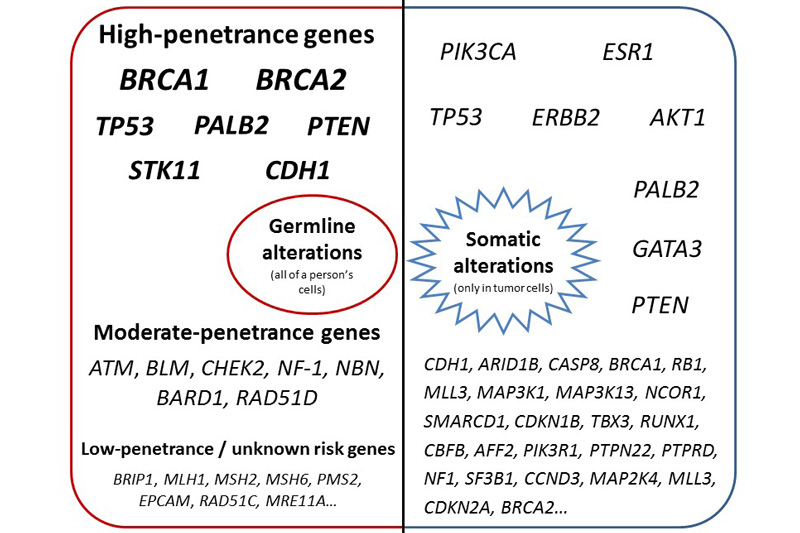
Fig. 1 Germline alterations: division according to the breast cancer susceptibility risk conferred by a mutation / alteration in each gene. High-penetrance genes: more than 4 fold increase in the risk of developing breast cancer, if mutated. Moderate-penetrance genes: 2-4 fold increase in risk. Low-penetrance genes: less than 2-fold increase in risk.
© Mariana Brandão, Christos Sotiriou.
Furthermore, there are several other genetic abnormalities that can moderately increase the risk of breast cancer (2 to 4 fold increase in risk), namely in ATM, BLM, CHEK2, NF-1, NBN, and BARD1 genes. Due to their prognosis value, there are specific guidelines for the management and follow-up of patients with these germline abnormalities, especially for the high-penetrance genes [8, 11, 12].
Yet, there are also germline abnormalities associated with a low (relative risk <2) or unknown breast cancer risk, namely BRIP1, RAD51C, RAD51D, MRE11A and mismatch repair genes (MLH1, MSH2, MSH6, PMS2, EPCAM). For these abnormalities, guidelines for follow-up are not so clear and usually patients are managed according to their family history. In addition, we still do not know the prognostic value of much of this sequenced DNA data, which have been leading to a rise in the number of “variants of unknownsignificance” (VUS) identified [1, 7, 8, 11]. As stated by ASCO and ESMO guidelines, it is often incorrect to change a patient’s clinical management based on the finding of a VUS [1, 8]. Furthermore, labs are encouraged to make genetic and clinical data publicly available, in order to study the clinical implications of the different genetic abnormalities and VUS. There are already public registries, like ENIGMA (https://enigmaconsortium.org) and PROMPT (http://promptstudy.org), but only a fraction of tested patients have their data deposited here.
Besides their prognostic value, germline mutations in the BRCA1/2 genes have predictive value, as they confer sensitivity to PARP inhibitors. There are already two agents (olaparib and talazoparib) approved by FDA for germline BRCA1/2-mutated patients in the advanced breast cancer (ABC) setting [13, 14]. These and other PARP inhibitors are currently being tested in the early setting. So far, no other germline alteration has proven to have predictive value in breast cancer.
Somatic mutations
Breast cancer subtypes present different mutational patterns, which influence response to treatment and prognosis [15]. Luminal A tumours present a higher proportion of PIK3CA mutations (49%), whereas basal-like tumours have mostly TP53 mutations (84%).
It has been shown that PIK3CA mutations have prognostic value as, in the early setting, they are associated with an improved invasive disease-free survival [16]. Yet, in HER2-positive tumours, they are correlated with a lower pathological complete response (pCR) rate [17, 18]. Regarding its predictive value to the use of PI3K inhibitors, results are more contradictory: in the early setting, the LORELEI trial (neoadjuvant letrozol with/without taselisib) showed similar benefit from the addition of taselisib (a PI3K-alfa inhibitor) in the overall population vs. in the PIK3CA-mutated subgroup [19]. In the metastatic setting, patients with a PIK3CA-mutated tumour presented similar hazard ratios for progression-free survival (PFS) compared to the wild-type/intention-to-treat population in the FERGI (fulvestrant with/without pictilisib, a pan-PI3K inhibitor) and PEGGY (paclitaxel with/without pictilisib) trials [20, 21]. On the other hand, in the BELLE-2 and BELLE-3 trials, only the subgroup of patients with a PIK3CA-mutated tumour benefited from the addition of buparlisib (a pan-PI3K inhibitor) [22, 23]. The SANDPIPER trial tested the addition of taselisib and SOLAR-1 tested the addition of alpelisib to endocrine treatment (ET) in two cohorts of patients: with and without PI3KCA-mutant tumours. In both trials, there was an increase in PFS only in patients with PIK3CA-mutant tumours [24, 25]. More recently, it has also been show a relatively frequent acquisition of new PIK3CA mutations in patients under ET or ET plus palbociclib [26], suggesting it can be a mechanism of resistance to ET.
It has also been shown that ESR1 mutations are a marker of resistance to ET, usually arising in patients treated with aromatase inhibitors in the adjuvant and metastatic settings [26–29]. Its detection can be used to monitor disease progression, and there is an ongoing trial (PADA-1, NCT03079011), testing the efficacy of a change in ET (aromatase inhibitor changed to fulvestrant) at the onset of detection of ESR1 mutations in the ctDNA of patients receiving palbociclib with an aromatase inhibitor.
Besides amplification, mutations in the HER2 (or ERBB2) gene have also been described in breast tumours. Yet, clinical data regarding the efficacy of anti-HER2 treatments in patients with HER2-mutated (non-amplified) breast cancer is limited [30].
Alterations in potential actionable genes in breast cancer have also been found in many other genes [15, 31]. Thus, using NGS, there are now several multigene panels that test breast tumours for multiple genetic alterations, like mutations and/or copy number alterations in PIK3CA, ERBB2, ESR1, TP53, GATA3, PTEN, CDKN2A, RB1, among others (Fig. 1). There are commercial tests that can be ordered by any clinician, such as Caris Molecular Intelligence (Caris Life Sciences, 592 genes) or FoundationOne CDx (Foundation Medicine, 324 genes and 2 genetic signatures). Some institutions have created their own multigene panels, like the Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT) assay (468 genes). Other institutions use commercial platforms such Ion AmpliSeq™ Cancer Hotspot Panel v2 (Thermo Fisher Scientific, 50 genes) or Oncomine Comprehensive Assay (Thermo Fisher Scientific, 161 genes in v3). There are two multigene panels approved by FDA (FoundationOne CDx [32] and MSK-IMPACT [33]), but in Europe, the assessment of genetic tests has traditionally been regulated mostly on the national level [4]. More recently, the European Network for Health Technology Assessment (EUnetHTA) has started to centrally perform health technology assessments. It has already reviewed prognostic tests for breast cancer recurrence, like Mammaprint®, OncotypeDX®, and FEMTELLE® [34], but no evaluation has yet been performed regarding multigene testing for mutations or other tumour’s genetic alterations. Furthermore, the clinical utility of these panels in breast cancer has not yet been proved [35].
In addition, patients with tumours with multiple alterations or with different abnormalities in each metastatic site are another challenge, as it must be decided which alteration to prioritize. Thus, a multianalyte test, including assessment of RNA and protein expression, may help in treatment decision, by clarifying which downstream pathway is activated. Furthermore, many institutions have already implemented Molecular Tumour Boards, to assist clinicians in the interpretation of these multigene panels’ results.
In addition, multigene panels allow grouping the tumour’s pattern of mutations, which is named a mutational signature. In breast cancer, defective DNA repair pathways (like mutations in BRCA1/2) cause homologous recombination deficiency (HRD) and, recently, it has been shown that somatic substitution, insertion/deletion and rearrangement patterns are also associated with HRD. Thus, a model called “HRDetect” was developed, which identifies homologous recombination-deficient tumours [36]. These tumours may also be sensitive to PARP inhibition. Using NGS, it is also possible to quantify the breast tumour’s mutational burden, which might be associated with response to immunotherapy [37, 38]. Yet, as stated, all of these markers need clinical validation in breast cancer. An exception is the infrequent detection of patients with breast tumours which are microsatellite instability (MSI)-high and, therefore, are candidates to treatment with immune checkpoint inhibitors [39].
When using this multigene panels for the detection of somatic abnormalities, clinicians should be aware that there is the potential for discovering alterations that may suggest germline susceptibility, like BRCA1/2 mutations [1]. These secondary findings should then be confirmed in DNA for normal cells, to assess if they are truly germline alterations.
Testing recommendations
There are multiple types of sequencing techniques, including targeted sequencing, whole exome sequencing (WES) and whole genome sequencing (WGS), better detailed in the “Multigene Sequencing for Treatment Selection: ESMO Biomarker Factsheet” [40]. A comparison of the advantages and disadvantages of each technique is provided in Table 1.
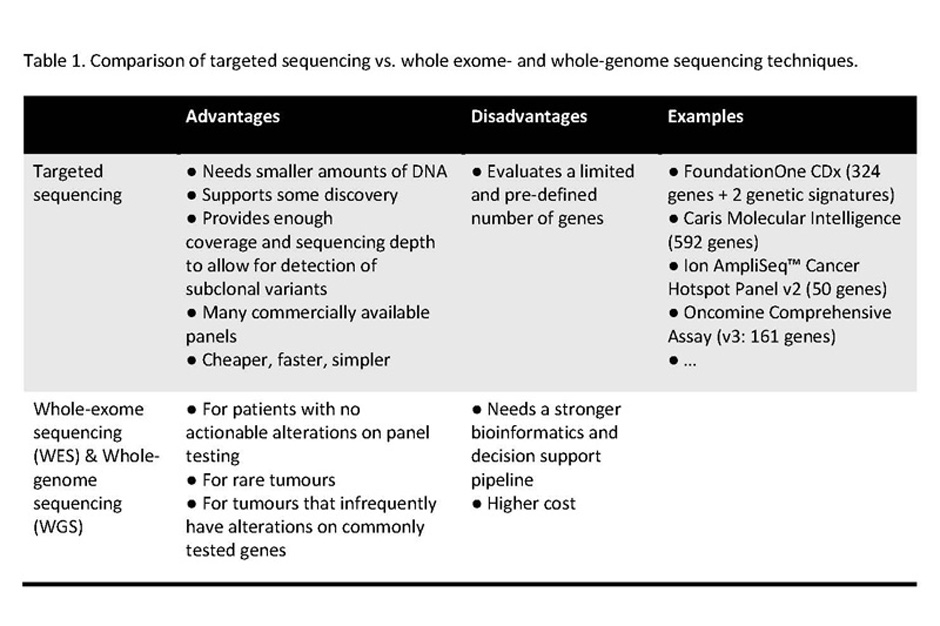
© Mariana Brandão, Christos Sotiriou.
Besides performing multigene sequencing in tumour tissue, it is also possible to perform it in ctDNA and CTCs. These so-called “liquid biopsies” have the advantage of being a non-invasive procedure, easily repeatable and highly reproducible and that can assess alterations in different malignant clones (tumour heterogeneity), allowing for a real-time monitoring of the disease [41]. However, they may miss small amounts of mutant DNA (e.g. subclonal alterations, low tumour burden…) and certain alteration types may be more difficult to detect (e.g. copy-number variations). Even so, liquid biopsies using multigene testing are being used for the inclusion of breast cancer patients with certain molecular alterations in clinical trials (e.g. plasmaMATCH trial, NCT03182634) and also for the monitoring of disease progression in trials (e.g. PADA-1 trial, NCT03079011) [42]. Nevertheless, if a known mutation is being followed through treatment (e.g. PIK3CAmut levels in ctDNA), a PCR-focused test is usually more cost-effective [31].
In the future, we will probably see an expansion of available biomarkers – besides multigene assessment, also transcriptional output, protein expression and epigenetic modifications may be evaluated (the “omics era”). This would provide a broader understanding of each tumour’s biology, potentially leading to better treatment decisions. At the same time, this would require powerful bioinformatics tools to analyse and interpret such a quantity of data.
It is also expected that both germline and somatic multigene testing will be done at the same time, especially for genes that are actionable for treatment (e.g. BRCA1/2 mutation).
Ensuring quality and timely testing results
In order to effectively apply multigene testing results to the care of the individual patient, these have to be available in a timely fashion and must comply with quality regulations – also better detailed in the “Multigene Sequencing for Treatment Selection: ESMO Biomarker Factsheet” [40]. This is especially the case for the detection of somatic alterations in the tumour, which can have a direct and immediate impact on treatment decision. Yet, nowadays, the detection of a germline BRCA1/2 mutation can also influence treatment in the metastatic setting and can lead to patient’s inclusion in clinical trials in the early setting. Thus, a timely result is paramount. Furthermore, the detection of a germline mutation can also change the surgical approach (breast conserving surgery vs. risk-reducing double mastectomy with/without oophorectomy), thus it is important to deliver these results within an adequate timing and ensure its quality.
Fortunately, turnaround times for multigene panels have decreased substantially over the past years and, nowadays, results are available within 10-21 days. Therefore, it is now possible to incorporate information regarding germline and somatic alterations into clinical decision-making at the time of breast cancer diagnosis.
Patient selection & applicability
When ordering a multigene panel test, the clinician must explain its purpose to the patient: if it is intended to assess breast cancer susceptibility risk (detection of germline alterations) and/or if it aims to tailor treatment (germline and/or somatic alterations).
Regarding the evaluation of breast cancer susceptibility risk, there are multiple criteria and guidelines to select and counsel patients [5, 6, 8, 11]. They are usually based on the patient’s age, family history of cancer, personal history of other cancers, breast tumour subtype, and presence of multifocal / bilateral breast tumour. Based on that, the clinician may request a limited test (e.g. only for mutations in the BRCA1/2 genes) or a multigene panel. As stated before, a problem associated with multigene testing is the detection of common low penetrance alleles associated with a slightly increased or decreased risk of breast cancer and, for which, no clear treatment / follow-up guidelines are available. On the other hand, as suggested by NCCN, multigene testing could be used “in patients who tested negative (or indeterminate) for one particular syndrome, but whose personal and family history is suggestive of an inherited susceptibility” [11]. Irrespective of the type of test requested, the patient should receive pre- and post-test counselling, and psychological support should be available to patients and their relatives [1, 5].
Information on germline alterations can also be used to tailor treatment, namely regarding surgery extent [12]. Furthermore, in terms of systemic treatment, patients with advanced HER2-negative breast cancer, not resistant to platinum drugs, and who have a germline BRCA1/2 mutation, are now eligible for treatment with PARP inhibitors, after previous treatment with taxanes and anthracyclines [13, 14]. In addition, in the early setting, these patients can be enrolled in clinical trials (e.g. OlympiA – NCT02032823). Thus, according to the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT), a germline BRCA1/2 mutation is a genomic alteration included in the tier I-A (“prospective, randomised clinical trials show the alteration-drug match in a specific tumour type results in a clinically meaningful improvement of a survival end point”) [43].
Regarding somatic multigene testing, its use in breast cancer is still controversial. The randomized SHIVA trial showed no benefit of using a matched molecularly targeted agent (outside their indications), as compared to treatment at physician’s choice, in patients with any kind of metastatic solid tumour refractory to standard of care [44]. Furthermore, in the SAFIR01 trial, directed solely to breast cancer and testing PIK3CA (exons 10 and 21) and AKT1 (exon 4), only 13% of the included patients received treatment directed by genomic alterations, which was lower than expected [45]. Some of the reasons to these disappointing results are intratumour heterogeneity, the lack of effective of drugs to most of the molecular targets so far, and the inclusion of a heterogeneous and heavily pre-treated population of patients. More recently, the MOSCATO trial, directed to patients with solid tumours, has found that 40% of included patients had an actionable molecular alteration, but only 19% were treated with a matched targeted therapy. A third of these treated patients had a 30% better PFS with the targeted therapy compared to the PFS with their previous treatment, which was encouraging. Yet, in the end, of the 1035 patients included, only 7% benefited from this molecularly targeted approach [46].
Thus, ASCO position statement and ESMO Advanced Breast Cancer (ABC) 4 guidelines state that multigene panels should not be used in routine clinical practice [1, 35]. Nevertheless, NGS testing can be applied to patients who are deemed fit to be included in clinical trials, e.g. within “prospective molecular triage programmes to select patients for therapeutic trials” [35].
As the pace of development is very fast and there are nowadays many multigene panels available, ESMO has created the aforementioned ESCAT scale, which aims to categorize the level of “actionability” of genetic mutations / alterations in a standardized way, in order to improve treatment-tailoring [43]. In breast cancer, besides germline BRCA1/2 mutations, only the amplification of ERBB2 (HER2) is included in the tier I-A. The results of SOLAR-1 have just been presented [25], but they may lead to the inclusion of a PIK3CA mutation in this tier as well, in the future. Then, on tier I-C (“clinical trials across tumour types or basket clinical trials show clinical benefit associated with the alteration-drug match, with similar benefit observed across tumour types”), there is mismatch repair deficiency (“MSI-high” tumours), as it is associated with benefit from the anti-PD1 checkpoint inhibitor pembrolizumab [39]. On tier III-B (“alteration that has a similar predicted functional impact as an already studied tier I abnormality in the same gene or pathway, but does not have associated supportive clinical data”) we have PALB2 loss-of-function mutations. The loss of PALB2 has a similar effect to BRCA2 loss-of-function, leading to defects in DNA repair. Therefore, patients with these altered tumours could potentially benefit from PARP inhibitors, but this needs to be tested in clinical trials.
At the moment, there are several clinical trials (e.g. NCI-MATCH [NCT02465060], TAPUR [NCT02693535], SAFIR02_Breast [NCT02299999], among others) and nation-wide projects, applying multigene sequencing to a number of different tumour types, including breast cancer. Furthermore, there are many online databases and public data resources, like the Cancer Genome Interpreter, cBioPortal, Catalog of somatic mutation in cancer (COSMIC), Clinical Interpretation of Variants in Cancer (CiVIC), among others, which perform annotation and analysis of tumour alterations data, and that can assist the physician in clinical-decision making [43].
In conclusion, the increasing use of multigene sequencing is changing the way we evaluate and treat breast cancer patients. Yet, there are many open questions regarding its utility and an intense research effort is being carried in this area.
References
- Robson ME, Bradbury AR, Arun B, et al. American Society of Clinical Oncology Policy Statement Update: Genetic and Genomic Testing for Cancer Susceptibility. JCO 2015; 33(31):3660–3667.
- Press Announcements - FDA authorizes, with special controls, direct-to-consumer test that reports three mutations in the BRCA breast cancer genes.
- Regulation (EU) 2017/746 of the European Parliament and of the Council of 5 April 2017 on in vitro diagnostic medical devices and repealing Directive 98/79/EC and Commission Decision 2010/227/EU (Text with EEA relevance. ), 2017.
- Kalokairinou L, Howard HC, Slokenberga S, et al. Legislation of direct-to-consumer genetic testing in Europe: a fragmented regulatory landscape. J Community Genet 2018; 9(2):117–132.
- Rutgers E, Balmana J, Beishon M, et al. European Breast Cancer Council manifesto 2018: Genetic risk prediction testing in breast cancer. European Journal of Cancer 2019; 106:45–53.
- Singer CF, Balmaña J, Bürki N, et al. Genetic counselling and testing of susceptibility genes for therapeutic decision-making in breast cancer—an European consensus statement and expert recommendations. European Journal of Cancer 2019; 106:54–60.
- Okur V, Chung WK. The impact of hereditary cancer gene panels on clinical care and lessons learned. Cold Spring Harb Mol Case Stud 2017. doi:10.1101/mcs.a002154.
- Paluch-Shimon S, Cardoso F, Sessa C, et al. Prevention and screening in BRCA mutation carriers and other breast/ovarian hereditary cancer syndromes: ESMO Clinical Practice Guidelines for cancer prevention and screening. Ann Oncol 2016; 27(suppl_5):v103–v110.
- Fountzilas C, Kaklamani VG. Multi-gene Panel Testing in Breast Cancer Management. In Gradishar WJ (ed): Optimizing Breast Cancer Management, Cham: Springer International Publishing, 2018:121–140.
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017; 317(23):2402–2416.
- NCCN Clinical Practice Guidelines in Oncology for Genetic/Familial High-Risk Assessment: Breast and Ovarian version 2.2019.
- NCCN Guidelines for Breast Cancer Risk Reduction version 2.2018.
- Robson M, Im S-A, Senkus E, et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. New England Journal of Medicine 2017; 377(6):523–533.
- Litton JK, Rugo HS, Ettl J, et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. New England Journal of Medicine 2018; 379(8):753–763.
- The Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature 2012; 490:61.
- Zardavas D, te Marvelde L, Milne RL, et al. Tumor PIK3CA Genotype and Prognosis in Early-Stage Breast Cancer: A Pooled Analysis of Individual Patient Data. JCO 2018; 36(10):981–990.
- Majewski IJ, Nuciforo P, Mittempergher L, et al. PIK3CA Mutations Are Associated With Decreased Benefit to Neoadjuvant Human Epidermal Growth Factor Receptor 2–Targeted Therapies in Breast Cancer. JCO 2015; 33(12):1334–1339.
- Fan H, Li C, Xiang Q, et al. PIK3CA mutations and their response to neoadjuvant treatment in early breast cancer: A systematic review and meta-analysis. Thorac Cancer 2018; 9(5):571–579.
- Saura C, de Azambuja E, Hlauschek D, et al. LBA10_PRPrimary results of LORELEI: A phase II randomized, double-blind study of neoadjuvant letrozole (LET) plus taselisib versus LET plus placebo (PLA) in postmenopausal patients (pts) with ER+/HER2-negative early breast cancer (EBC). Ann Oncol 2017. doi:10.1093/annonc/mdx440.001.
- Krop IE, Mayer IA, Ganju V, et al. Pictilisib for oestrogen receptor-positive, aromatase inhibitor-resistant, advanced or metastatic breast cancer (FERGI): a randomised, double-blind, placebo-controlled, phase 2 trial. The Lancet Oncology 2016; 17(6):811–821.
- Vuylsteke P, Huizing M, Petrakova K, et al. Pictilisib PI3Kinase inhibitor (a phosphatidylinositol 3-kinase [PI3K] inhibitor) plus paclitaxel for the treatment of hormone receptor-positive, HER2-negative, locally recurrent, or metastatic breast cancer: interim analysis of the multicentre, placebo-controlled, phase II randomised PEGGY study. Ann. Oncol. 2016; 27(11):2059–2066.
- Baselga J, Im S-A, Iwata H, et al. Buparlisib plus fulvestrant versus placebo plus fulvestrant in postmenopausal, hormone receptor-positive, HER2-negative, advanced breast cancer (BELLE-2): a randomised, double-blind, placebo-controlled, phase 3 trial. The Lancet Oncology 2017; 18(7):904–916.
- Di Leo A, Johnston S, Lee KS, et al. Buparlisib plus fulvestrant in postmenopausal women with hormone-receptor-positive, HER2-negative, advanced breast cancer progressing on or after mTOR inhibition (BELLE-3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2018; 19(1):87–100.
- Baselga J, Dent SF, Cortés J, et al. Phase III study of taselisib (GDC-0032) + fulvestrant (FULV) v FULV in patients (pts) with estrogen receptor (ER)-positive, PIK3CA-mutant (MUT), locally advanced or metastatic breast cancer (MBC): Primary analysis from SANDPIPER. JCO 2018; 36(18_suppl):LBA1006–LBA1006.
- André F, Ciruelos EM, Rubovszky G, et al. LBA3_PRAlpelisib (ALP) + fulvestrant (FUL) for advanced breast cancer (ABC): Results of the phase III SOLAR-1 trial. Ann Oncol 2018. doi:10.1093/annonc/mdy424.010.
- O’Leary B, Cutts RJ, Liu Y, et al. The genetic landscape and clonal evolution of breast cancer resistance to palbociclib plus fulvestrant in the PALOMA-3 trial. Cancer Discov 2018. doi:10.1158/2159-8290.CD-18-0264.
- Allouchery V, Beaussire L, Perdrix A, et al. Circulating ESR1 mutations at the end of aromatase inhibitor adjuvant treatment and after relapse in breast cancer patients. Breast Cancer Research 2018; 20(1):40.
- Angus L, Beije N, Jager A, et al. ESR1 mutations: Moving towards guiding treatment decision-making in metastatic breast cancer patients. Cancer Treatment Reviews 2017; 52:33–40.
- Kuang Y, Siddiqui B, Hu J, et al. Unraveling the clinicopathological features driving the emergence of ESR1 mutations in metastatic breast cancer. npj Breast Cancer 2018; 4(1):22.
- Connell CM, Doherty GJ. Activating HER2 mutations as emerging targets in multiple solid cancers. ESMO Open 2017. doi:10.1136/esmoopen-2017-000279.
- Kurnit KC, Dumbrava EEI, Litzenburger B, et al. Precision Oncology Decision Support: Current Approaches and Strategies for the Future. Clin. Cancer Res 2018; 24(12):2719–2731.
- Recently-Approved Devices - FoundationOne CDx - P170019.
- In Vitro Diagnostics - Nucleic Acid Based Tests.
- Prognostic tests for breast cancer recurrence (PTBCR) – EUnetHTA.
- Cardoso F, Senkus E, Costa A, et al. 4th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 4). Ann. Oncol. 2018. doi:10.1093/annonc/mdy192.
- Davies H, Glodzik D, Morganella S, et al. HRDetect is a predictor of BRCA1 and BRCA2 deficiency based on mutational signatures. Nature Medicine 2017; 23(4):517–525.
- Goodman AM, Kato S, Bazhenova L, et al. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol Cancer Ther 2017; 16(11):2598–2608.
- Tumour Mutational Load: ESMO Biomarker Factsheet | OncologyPRO.
- Le DT, Uram JN, Wang H, et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med 2015; 372(26):2509–2520.
- Multigene Sequencing for Treatment Selection: ESMO Biomarker Factsheet | OncologyPRO.
- Ignatiadis M, Dawson S-J. Circulating tumor cells and circulating tumor DNA for precision medicine: dream or reality? Ann Oncol 2014; 25(12):2304–2313.
- O’Leary B, Hrebien S, Morden JP, et al. Early circulating tumor DNA dynamics and clonal selection with palbociclib and fulvestrant for breast cancer. Nat Commun 2018; 9(1):896.
- Mateo J, Chakravarty D, Dienstmann R, et al. A framework to rank genomic alterations as targets for cancer precision medicine: the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT). Ann Oncol 2018; 29(9):1895–1902.
- Le Tourneau C, Delord J-P, Gonçalves A, et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. The Lancet Oncology ; 16(13):1324–1334.
- André F, Bachelot T, Commo F, et al. Comparative genomic hybridisation array and DNA sequencing to direct treatment of metastatic breast cancer: a multicentre, prospective trial (SAFIR01/UNICANCER). The Lancet Oncology 2014; 15(3):267–274.
- Massard C, Michiels S, Ferté C, et al. High-Throughput Genomics and Clinical Outcome in Hard-to-Treat Advanced Cancers: Results of the MOSCATO 01 Trial. Cancer Discov 2017; 7(6):586–595.
Declaration of interest
Mariana Brandão has reported:
Research grants to institute: Roche, Menarini Silicon Biosystems, Janssen Diagnostics.
Christos Sotiriou has reported:
Advisory Boards of Astellas, Cepheid, Vertex, Seattle Genetics, Puma.
Participation in a company sponsored speakers bureau of Eisai, prIME Oncology, Teva, Foundation Medicine.
Other support from Roche, Genentech and Pfizer.

