

Definition of HER2
The human epidermal growth factor receptor 2 (HER2) is a transmembrane receptor tyrosine kinase located on chromosome 17q21. It is a member of the epidermal growth factor receptor (EGFR) family, which includes also EGFR (HER1), HER3, and HER4. In normal cells, activation of HER2 via homo- or hetero-dimerisation mediates cell signalling pathways including the phosphatidylinositol 3-kinase (PI3K)/protein kinase B (AKT)/mammalian target of rapamycin (mTOR) and mitogen-activated protein kinase (MAPK) pathways, which regulate cellular processes of proliferation, motility and survival.
HER2 acts as an oncogene in breast cancer, its overexpression resulting in ligand-independent dimerisation which leads to constitutive activation of its cytoplasmic kinase domain.1 This constitutive activation of HER2 leads to un-regulated activation of the PI3K/AKT/mTOR and MAPK pathways, which promotes uncontrolled cell proliferation, evasion of apoptosis, angiogenesis, and invasion, leading to tumour growth and progression.
HER2 Expression in Breast Cancer
Oncogenic HER2 is overexpressed in 15-20% of primary breast cancers2 and in approximately 10% of ER-positive breast cancers.3 Overexpression of HER2 in breast cancer occurs predominantly through amplification of the HER2 gene and is associated with a more aggressive phenotype.4,5 Amplification of the gene leads to high-level expression driving the basal level of HER2 activity above a threshold that can stimulate tumour growth.1
Discovery of the HER2 oncogene led to the development of one of the first approved humanised monoclonal antibody-based targeted therapy, trastuzumab, revolutionising breast cancer management.
HER2 as a Prognostic Biomarker in Breast Cancer
The potential of HER2 as a prognostic biomarker in breast cancer was first reported in 1987, with its amplification associated with reduced time to progression and reduced overall survival.5 Many subsequent studies have confirmed this link with poor prognosis and demonstrated an association of HER2-positivity with high grade tumours, lymph node involvement, and a higher rate of disease recurrence and mortality.6 HER2 overexpression/amplification has also been associated with poorer outcomes in node-negative breast cancer patients.7
HER2 as a Predictive Biomarker in Breast Cancer
HER2 is an important predictive biomarker of response to HER2-targeted therapies, including trastuzumab, lapatinib, pertuzumab, and trastuzumab emtansine (T-DM1). HER2-positivity is also associated with greater response to chemotherapeutic agents including anthracyclines and taxanes and with poorer response to endocrine therapies.4
Trastuzumab is a humanized monoclonal antibody that targets the extracellular domain of HER2, blocking its activation, and has demonstrated significant survival benefit when used first line or in an adjuvant setting in patients with HER2-positive tumours. Trastuzumab has European approval for the treatment of early-stage and metastatic HER2-positive breast cancer based on clinical trials that have demonstrated improved response rates, and reduced risk of recurrence and mortality when this drug is used as monotherapy or in combination with chemotherapy in early stage and metastatic breast cancer expressing HER2.8-10 Long-term follow-up of two randomised trials demonstrated that adjuvant trastuzumab sustains both a significant disease free and overall survival benefit compared with chemotherapy alone.11
Lapatinib is a small molecule inhibitor of the kinase activity of HER2 and EGFR that has demonstrated clinical benefit as monotherapy or in combination with chemotherapy or trastuzumab in patients with HER2-positive metastatic breast cancer.12-14 Lapatinib has European approval for the treatment of HER2-positive breast cancer, used in combination with capecitabine for patients with advanced or metastatic disease that have progressed on prior chemotherapy or trastuzumab, in combination with trastuzumab for patients with hormone receptor-negative metastatic disease that have progressed on prior trastuzumab therapies in combination with chemotherapy, or in combination with an aromatase inhibitor for postmenopausal women with hormone receptor-positive metastatic disease.15
Pertuzumab is monoclonal antibody that binds to extracellular domain of HER2 inhibiting its activation. This drug has European approval for use in combination with docetaxel and trastuzumab for the treatment of patients with HER2-positive metastatic or locally recurrent unresectable breast cancer, who have not received previous anti-HER2 therapy or chemotherapy for their metastatic disease.16 The randomised, phase III clinical trial, CLEOPATRA, of 808 patients with HER2-positive metastatic breast treated first-line with pertuzumab plus trastuzumab and docetaxel versus trastuzumab plus docetaxel demonstrated significant improvement in median progression-free survival of 18.5 versus 12.4 months, respectively.17
Trastuzumab emtansine is an antibody drug conjugate in which trastuzumab is linked to the microtubule-inhibitory agent emtansine (DM1). In a randomised phase III clinical trial, trastuzumab emtansine plus capecitabine was associated with significantly prolonged progression-free survival and overall survival compared with lapatinib plus capecitabine.18 Trastuzumab emtansine is approved in Europe as monotherapy for the treatment of adult patients with HER2-positive, unresectable locally advanced or metastatic breast cancer previously treated with trastuzumab and taxane, separately or in combination.19
HER2 Testing Recommendations in Breast Cancer
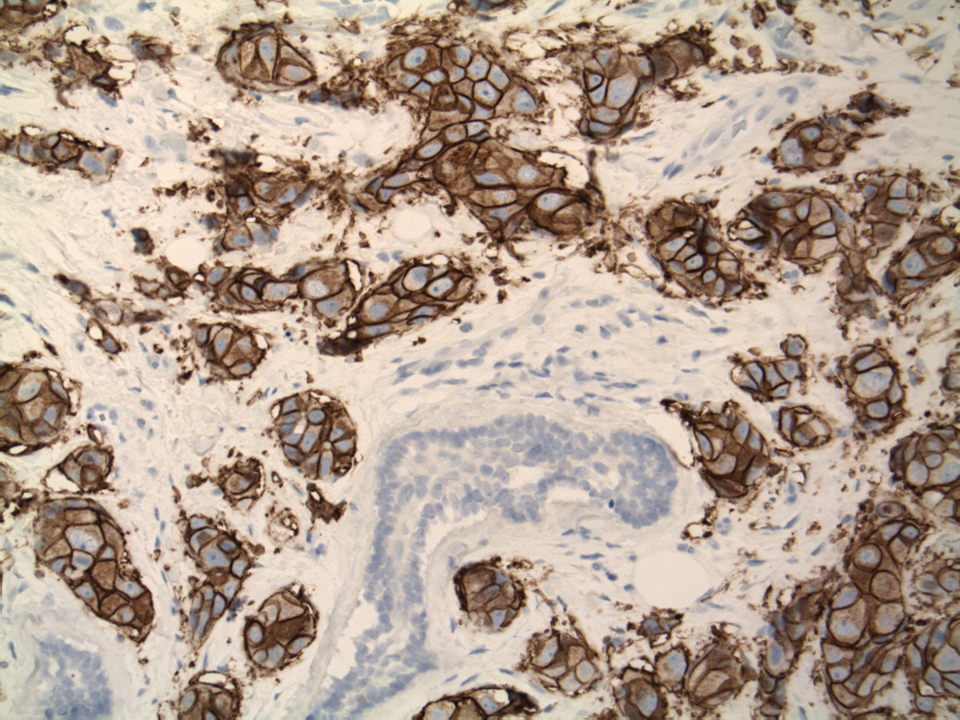
Intense and complete immunostaining for HER2 (score 3+) in invasive breast carcinoma. The normal breast duct does not show any membrane staining.
Credit: Giuseppe Viale
HER2 testing can be performed by either immunohistochemistry (IHC), or in situ hybridization (ISH) using either fluorescent (FISH), chromogenic (CISH) or silver (SISH) detection methods. These tests are generally carried out on core biopsy or resected tumour tissue samples that are fixed in buffered formalin and embedded in paraffin wax.
IHC detects HER2 protein expression and there are a number of antibodies commercially available for this type of assay.
ISH can detect the presence or absence of specific DNA sequences on chromosomes using complementary probes that hybridise to the region of interest. HER2 copy number can be assessed with ISH using either a single-probe or dual-probe assay. A single-probe assay measures only HER2 copy number and amplification is defined by examining the average HER2 copy number. A dual-probe assay measures both HER2 and chromosome 17 copy number and amplification is defined by examining both the HER2/Chr17 ratio and the average HER2 copy number.2
Scoring Recommendations
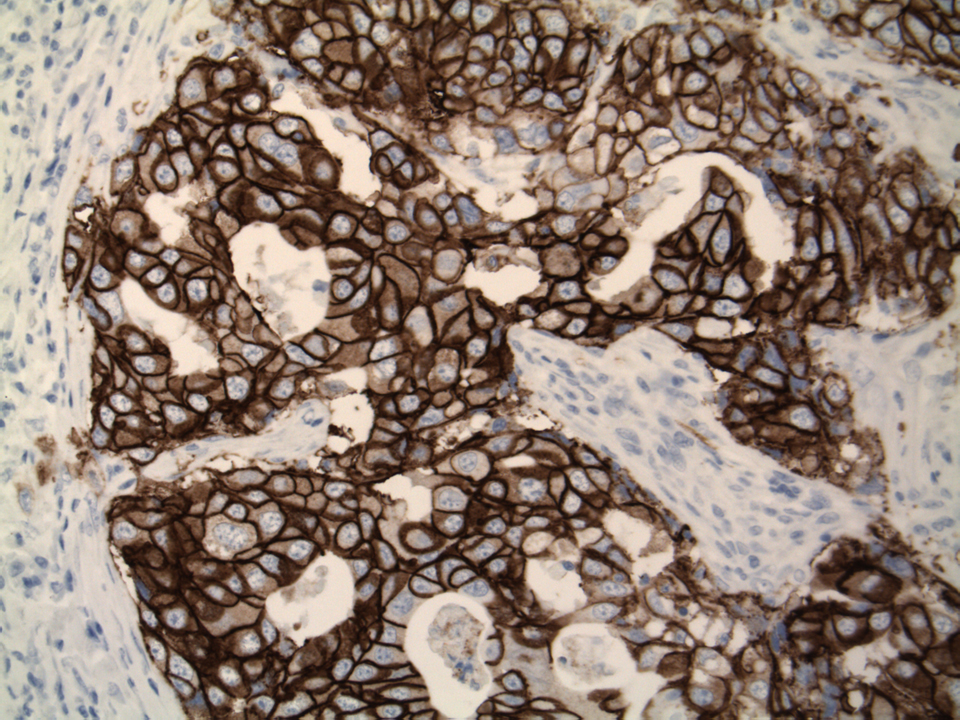
Intense and complete immunostaining for HER2 (score 3+) in invasive breast carcinoma. In addition to membrane staining, a weaker cytoplasmic staining is also present.
Credit: Giuseppe Viale
IHC: Scoring of HER2 is graded as 0 to 3+, based on an assessment of the intensity of the reaction product, the completeness of membrane staining, and the percentage of positive cells.2,6 An IHC score of 3+ is categorised as HER2 positive and is defined as strong complete reactivity seen in >10% of tumour cells. An IHC score of 2+ is classified as borderline reactivity (equivocal) and defined as weak to moderate complete membranous reactivity in >10% of tumour cells. IHC scores 0 and 1+ are considered HER2 negative. IHC 1+ is defined as faint, barely perceptible membranous reactivity in >10% of tumour cells. IHC 0 is defined as no reactivity or membranous reactivity in <10% of tumour cells.
For single-probe ISH FISH, HER2 positivity can be defined as an average copy number ≥6 signals/cell.2 An average copy number ≥4 to <6 is deemed equivocal and an average copy number <4 is considered HER2-negative. For dual-probe ISH, HER2 positivity is defined as a HER2/Chr17 ratio >2 or a ratio <2 with an average HER2 copy number ≥6 signals/cell. A ratio <2 with an average copy number ≥4 to <6 is deemed equivocal and a ratio <2 with an average copy number <4 is considered HER2-negative.
Ensuring Quality and Timely HER2 Testing Results
Erroneous or inconclusive HER2 test results may lead to inappropriate patient management. The American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) have produced a comprehensive set of guidelines of recommendations to improve the accuracy of HER2 testing and its utility as a predictive marker in invasive breast cancer.2 To ensure accurate and reproducible results HER2 testing must be determined using an accurate and validated assay performed in a specialised laboratory, which can ensure validation of the testing procedures. As well as performing initial test validation, a laboratory performing HER2-testing must adhere to ongoing internal quality assurance, ongoing external proficiency testing, and routine periodic performance monitoring. There should be comprehensive standardisation of methodology, validated controls and validated scoring procedures and the laboratory should participate in a relevant accreditation scheme such as the UK National External Quality Assessment Scheme (NEQAS).2,6 Ideally, a CE-marked in vitro diagnostic medical device should be used, but if not available, HER2-status should be assessed by an alternate prospectively validated test.
It is recommended that specimen fixation is performed quickly (time to fixation within 1 hour) and that the specimen is fixed in 10% neutral buffered formalin for 6 to 72 hours.2 Repeat testing should be considered if results seem discordant with other histopathology findings.
Which Technique and Which Algorithm Should be Used for the Analysis of the HER2 Status in Breast Cancer?
European licences for HER2 targeted therapies define HER2-positivity as a 3+ score by IHC and/or a positive result by ISH8,15-16,19 The European Society for Medical Oncology (ESMO) clinical practice guidelines for breast cancer management state that HER2 status can be determined by IHC or ISH and that ISH testing should be performed for tumours with an ambiguous (2+) IHC score.20
Patient Selection
Early and accurate HER2 testing of all breast cancer patients at primary diagnosis is essential for optimal disease management.6 It is recommended that HER2 status (HER2 negative or positive) be determined in all patients with invasive (early stage or recurrence) breast cancer on the basis of one or more HER2 test results.2,20 HER2 targeted therapy is recommended in all breast cancer patients testing positive for HER2 overexpression/amplification.2
References
- Leong AS-Y and Zhuang Z. The Changing Role of Pathology in Breast Cancer Diagnosis and Treatment. Pathobiology 2011; 78(2): 99–114.
- Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol 2013;31(31):3997-4013.
- De Abreu FB, Schwartz GN, Wells WA, Tsongalis GJ. Personalized therapy for breast cancer. Clin Genet 2014;86(1):62-7.
- Patani N, Martin LA, Dowsett M. Biomarkers for the clinical management of breast cancer: international perspective. Int J Cancer 2013;133(1):1-13.
- Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human Breast Cancer: Correlation of Relapse and Survival with Amplification of the HER-2/neu Oncogene. Science 1987;235:177-182.
- Payne SJ, Bowen RL, Jones JL, Wells CA. Predictive markers in breast cancer--the present. Histopathology 2008;52(1):82-90.
- Chia S, Norris B, Speers C, et al. Human epidermal growth factor receptor 2 overexpression as a prognostic factor in a large tissue microarray series of node-negative breast cancers. J Clin Oncol 2008;26(35):5697-704.
- Trastuzumab. Summary of Product Characteristics. 2015.
- Nahta R. Molecular Mechanisms of Trastuzumab-Based Treatment in HER2-Overexpressing Breast Cancer. ISRN Oncol 2012;2012:428062.
- Slamon DJ, Leyland-Jones B, Shak S, et al. Use of Chemotherapy plus a Monoclonal Antibody against HER2 for Metastatic Breast Cancer That Overexpresses HER2. N Engl J Med 2001;344:783-79.
- Perez EA, Romond EH, Suman VJ, et al. Four-Year Follow-Up of Trastuzumab Plus Adjuvant Chemotherapy for Operable Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer: Joint Analysis of Data From NCCTG N9831 and NSABP B-31. J Clin Oncol 2011;29(25):3366-73.
- Geyer CE, Forster J, Lindquist D, et al. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med 2006;355(26):2733-43.
- Blackwell KL, Burstein HJ, Storniolo AM, et al. Randomized study of Lapatinib alone or in combination with trastuzumab in women with ErbB2-positive, trastuzumab-refractory metastatic breast cancer. J Clin Oncol 2010;28(7):1124-30.
- Toi M, Iwata H, Fujiwara Y, et al. Lapatinib monotherapy in patients with relapsed, advanced, or metastatic breast cancer: efficacy, safety, and biomarker results from Japanese patients phase II studies. Br J Cancer 2009;101(10):1676-82.
- Lapatinib. Summary of Product Characteristics. 2015.
- Pertuzumab. Summary of Product Characteristics. 2015.
- Baselga J, Cortés J, Kim SB, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med 2012;366(2):109-19.
- Verma S, Miles D, Gianni L, et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med 2012;367(19):1783-91.
- Trastuzumab emtansine. Summary of Product Characteristics. 2014.
- Senkus E, Kyriakides S, Penault-Llorca F, et al. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2013;24(Suppl 6):vi7-23.
