

Definition of ALK
The ALK (anaplastic lymphoma kinase) gene is located at 2p23.1 on the short arm of chromosome 2. The ALK protein product of the gene is a member of the insulin super group of receptor tyrosine kinases. ALK is membrane bound and whilst there are a number of postulated ligands, including pleiotrophin and midkine (polypeptide nerve growth factors), there is little known about this aspect of ALK biology. ALK activation signals downstream in cells, activating PI3 kinase, but is also capable of activating the RAS/RAF/MAPK and the JAK/STAT pathways.
The physiological functions of ALK are little known but there appears to be a role in neonatal nervous system development and neurogenesis, at least in mouse models. In many ways, the downstream effects of the activated ALK kinase may be similar to those of activated EGFR and are the basis of the oncogenic effect of excess ALK activation.
ALK Abnormalities in NSCLC
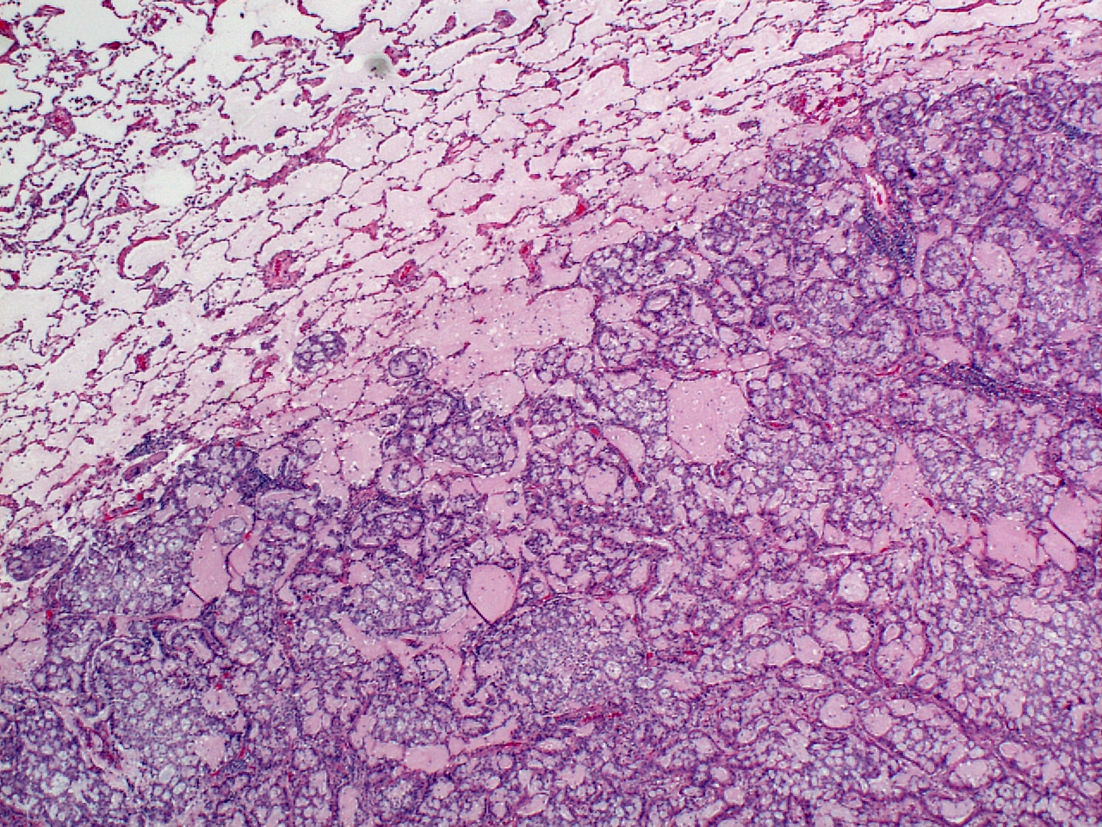
An haematoxylin and eosin stained cribriform pattern lung adenocarcinoma.
Credit: Keith Kerr
Abnormalities of ALK biology have been known in lymphomas (hence the name) and in some other human tumours, for some time. As recently as 2007, however, a translocation involving the ALK gene and EML4, was discovered in non-small cell lung cancer (NSCLC). An inversion in chromosome 2p placed the 5’ end of the EML4 gene next to the 3’ end of the ALK gene. The resulting fusion gene product included an activated ALK kinase which was active, independent of ligand binding. Various animal models were used to demonstrate the oncogenic, transforming properties of the fusion gene, as well as the possibility of abolishing oncogenic activity and suppressing tumour growth using an ALK tyrosine kinase inhibitor (ALK TKI). Subsequently, a range of different segments of the EML4 gene have been identified as variant partners for the same 3’ sector of the ALK gene in human clinical cases. In addition, other genes in other chromosomes (KIF5B, KCL1, TFG and, in a different rearrangement, PTPN3) may act as partner in a translocation, also leading to a fusion gene whose product has an activated ALK kinase.
The reported prevalence of ALK gene rearrangements (inversions involving EML4 being much commoner than the other translocations) in NSCLC is highly variable and is directly dependent upon the population tested. Selection of cases using clinical criteria associated with higher prevalence bias some studies towards higher figures. Like EGFR mutation, ALK rearrangement is not driven by tobacco carcinogenesis, so is commoner in never smokers but there is no reason why an individual smoker may not develop such a tumour. Patients with ALK rearranged tumours have a tendency to be younger than average lung cancer patients (mid-50s) but the gender differences seen in EFGR mutation are generally not found in ALK positive cases. Case selection on the basis of histology also has dramatic effect on results. Once again, like EGFR mutation, ALK fusion is a biological characteristic of non-tobacco driven carcinogenesis in the peripheral lung epithelium, the terminal respiratory unit (TRU) and is therefore a feature of adenocarcinomas. If all NSCLCs are tested for ALK fusions the prevalent outcome will be much lower, depending on the proportion of squamous cell carcinomas in the test population. Rare ALK rearranged squamous cell carcinomas are reported but these cases are exceptional, and if encountered, the first matter should be to question the histological diagnosis. With all these caveats, reported prevalence ranges from approximately 2-7% of non-squamous NSCLC cases.
ALK as a Predictive Biomarker in Lung Cancer
So far, there are no established data to suggest there is any difference, clinically or in therapeutic response to ALK TKIs, between the different fusion proteins reported. In the vast majority of the studies, however, the partner of the ALK gene is unknown since the method used to detect the rearrangement is a break-apart fluorescence in situ hybridization (FISH) test (see below). Studies have consistently shown a 60-70% response rate (RECIST) to ALK TKI therapy in ALK rearranged NSCLC.
ALK Testing in NSCLC
Most guidelines recommend that all patients with a definite, probable or possible adenocarcinoma should have their tumour tested for ALK gene rearrangement. In never or long time ex-smokers it is reasonable to consider testing squamous cell carcinomas.
Clinical parameters – smoking habit, gender, age, ethnicity etc. should not be used to select patients for testing. Excluding smokers with adenocarcinoma would risk missing a substantial proportion of treatable mutations.
Although ALK TKI therapy is generally the preserve of stage IV disease, and is currently only licensed for second or greater lines of therapy, testing is often carried out regardless of stage, for practical purposes, or in the absence of stage information. Reflex testing, driven by the pathologist on making the appropriate histological diagnosis, is widely practice but, for a variety of reasons, local practice may favour ‘bespoke’ testing driven on request by the oncologist or tumour board. It is sometimes debated that when the drug is given in second line, it is inappropriate to test for ALK ‘upfront’ at initial diagnosis. In the authors view, it is more practical to test for all relevant markers at initial diagnosis. Some oncologists express a preference for knowing a patient is ALK rearranged whilst they are receiving their first line chemotherapy. This dynamic will change as ALK TKIs find their way into first line use.
Testing Methodology
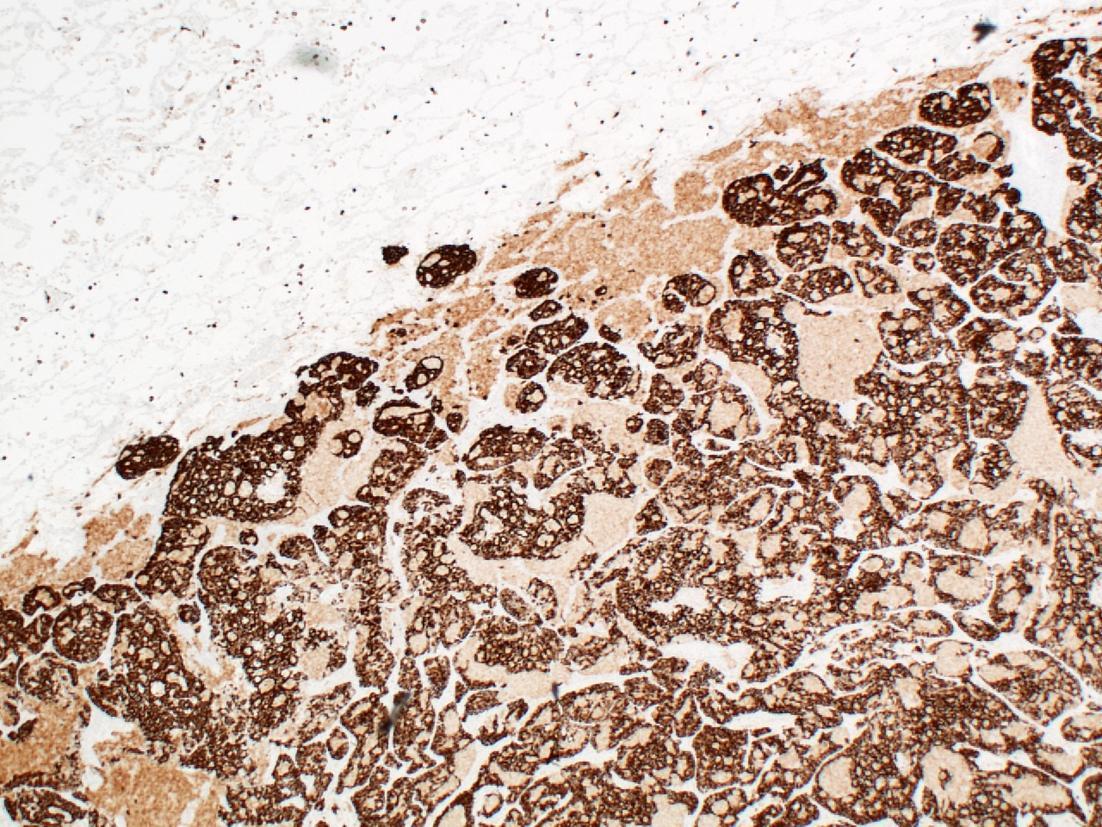
ALK immunohistochemistry using the Ventana D5F3 immunohistochemistry kit.
Credit: Keith Kerr
There are several different methods that have been used to identify patients whose tumours harbour an ALK gene rearrangement and there is still little clear consensus over how testing should be approached. The traditional laboratory approach to detecting gene rearrangements has been a fluorescence in situ hybridisation (FISH) based assay. Fusion gene mRNA gene product may be identified by a reverse transcriptase polymerase chain reaction (RT-PCR) assay and various approaches to massive parallel sequencing (Next Generation Sequencing – NGS) can identify fusion genes at the DNA level. Of course, it is the abnormal ALK protein product of the fusion gene which exerts oncogenic activity and ALK gene rearrangements in NSCLC are associated with modest elevations of ALK protein in tumour cells, which may be detected by immunohistochemistry (IHC).

Positive ALK FISH test. There are fused or proximate signals but extra ‘single red’ signals. This latter feature is found in around 30% of ALK gene rearrangements when there is apparent loss of the 5’ (green) probe signal.
Credit: Keith Kerr
FISH testing using dual colour break apart probes is still regarded as the ‘gold standard’ test, largely because this traditional approach was used, and therefore validated, in the early clinical trials of crizotinib in ALK rearranged NSCLC. The FISH test was subsequently approved as the companion diagnostic to crizotinib therapy by the US FDA, and so it remains to date. This FISH test requires a minimum read on at least 50 assessable cells, at least 50% of which should show non-fused ALK genes as highlighted by either separation of the 3’ and 5’ probes by 2 or more diameters of the fluorescent signal or loss of the 5’ signal. If less than this % of abnormal cells are found, two readers should assess 100 cells and the average score of abnormal cells should exceed 15% - a somewhat arbitrary figure which accounts for cutting artefacts and various other sporadic events which are not indicative of an ALK gene rearrangements. FISH is relatively expensive and time consuming, requires special expertise and equipment and ALK FISH in particular can be challenging to read. The paucity of tumour cells in many lung cancer samples also makes reading FISH difficult. Chromogenic in situ hybridisation (CISH) is now available for ALK testing. This has the advantage of using bright field microscopy so morphology is better preserved, but experience with this technique is limited.
RT-PCR is a very specific technique, but it lacks sensitivity and reliability. Rare fusion genes may be missed if the primer set for the multiplex PCR reaction does not cover the fusion gene in question, and quality mRNA may not be available from formalin fixed paraffin embedded (FFPE) tissue, the usual source of lung cancer diagnostic material. Failure rates of up to 30% on FFPE tissue are reported. This technology is not widely available and requires special expertise. Cost is moderate.
Detection of fusion genes using NGS approaches is feasible but not widely practiced in the routine clinical setting. Undoubtedly, as technology and experience improve, this approach will be widely adopted. Whether this test will be adopted as the primary diagnostic or as a screening tool, requiring confirmation by FISH or IHC, remains to be seen.
IHC to detect elevated levels of ALK protein is an extremely effective surrogate marker of ALK gene rearrangement. Many laboratories use ALK IHC as a cheap, rapid screening method to identify possible cases for subsequent confirmation by either FISH of, less often, RT-PCR. IHC is, however, becoming established as a primary predictive selector for ALK TKI therapy in Europe and Asia where regulatory authorities are less proscriptive about the nature of an ‘ALK test’ that may be used to select patients for such treatment. Several adequate ALK IHC antibodies are available but, for successful testing, it is essential that an adequately sensitive IHC detection system is used in order that the modest elevations in ALK protein may be detected. There has been much discussion around the issue of non-correlative ALK IHC and FISH (one modality positive, the other negative). Whilst true examples undoubtedly exist, they are probably rare (<5% of all cases with an abnormal ALK test), most discrepant test combinations are probably so for technical reasons. There are reports of ALK IHC positive, ALK FISH negative tumours responding to ALK TKIs and there has been anecdotal reporting that tumours with the reverse discrepant test findings respond less well to crizotinib which makes intuitive sense, since the protein exerts oncogenic influence and is the target of the drug.
Samples for Testing
Any pathological samples containing tumours cells may be used: biopsy samples, cytology material, surgically resected tumour. Whilst samples for FISH require a minimum number of assessable tumour cells, and both RT-PCR and NGS techniques depend to mRNA or DNA quality and quantity, ALK IHC may be read on a very small number of cells. To the best of our knowledge, heterogeneity of expression is not a major confounder of these tests but data are limited. Depending on the IHC technology used, pathologists must be aware of the pitfalls of testing, as they must when reading FISH tests, in order to avoid false positive or false negative results.
Ensuring Timely and Quality ALK Testing
There are many steps and many individuals involved in the work chain from the decision to test, through sample handling, submission to the molecular lab, assimilation of the molecular and pathological data and reporting back to the treating physician. IHC can be carried out and read in a number of hours – a same day service may be feasible, a next day service quite routine. FISH testing usually takes longer. Currently NGS test results can take many days to be verified. Efficient communication and working systems are vital for timely diagnosis. These details are moot while ALK TKIs are only available in the second or greater lines of therapy but become more critical for first line treatment decisions or when testing is deferred until second line.
All labs issuing clinical reports should participate in, and perform adequately in external quality assurance programmes. Regular in-house monitoring of performance, and awareness of potential false positive and false negative tests is important.
Reporting ALK Test Results
ALK test results should be reported in the context of the sample which was diagnosed with NSCLC and assimilated into the overall pathology report. Context is vital, to avoid misinterpretation of results. Expert pathologist input is required for FISH test assessment, since identification of tumour cells is challenging.
Pathologists should be aware of the possibility of positive ALK IHC in lung neuroendocrine tumours in the absence of a positive FISH test. The significance of such findings is unclear.
The report to the treating physician should provide detail of the ALK test methodology used and, in the case of the FISH test, the number of cells assessed and the % showing abnormalities indicating a non-fused ALK gene. Generic comments about the implications of any findings for therapy are acceptable, but specific treatment recommendations should be avoided.
References
- Ou S-H I, Bartlett C, Mino-Kenudson M, et al. Crizotinib for the treatment of ALK-rearranged non-small cell lung cancer: A success story to usher in the second decade of molecular targeted therapy in oncology. The Oncologist 2012;17, 1351-1375.
- Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature 2007; 448, 561-566.
- Rikova K, Guo A, Zeng Q, et al. Global survey of phosphotyrosine signalling identifies oncogenic kinases in lung cancer. Cell 2007; 131, 1190-1203.
- IASLC Atlas of ALK testing in lung cancer. Tsao MS, Hirsch FR, Yatabe Y (Eds). International association for the study of lung cancer, Colorado, USA. October 2013.
- Kerr KM. ALK Testing in Non-Small Cell Lung Carcinoma: What Now? J Thorac Oncol 2014;9:593-595.
- Lindeman NI, Cagle PT, Beasley MB, et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Thorac Oncol 2013;8:823-59
- Kerr KM, Bubendorf L, Edelman MJ, et al. Second ESMO Consensus Conference on Lung Cancer: pathology and molecular biomarkers for non-small-cell lung cancer. Ann Oncol 2014; 25, 1681-90.
